点评
感谢阿Q的翻译!这里的media是指培养基,前面有提到使用获取自小鼠模型上的耐药细胞进行培育。
| |
| |
 求助贴,奥西替尼一年多后CT有进展,
我父亲今年79,23年12月穿刺病理诊断为肺腺癌晚期。
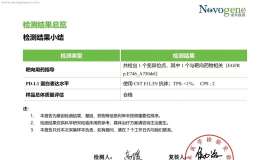
基因检测EGRF19外显因子突变,丰
求助贴,奥西替尼一年多后CT有进展,
我父亲今年79,23年12月穿刺病理诊断为肺腺癌晚期。
基因检测EGRF19外显因子突变,丰
 “砰”!国产新药获批,击穿肺癌靶向
作者:Tony
与欧美人种不同的是,亚洲肺癌患者EGFR突变率高,约达到50%[1],有更多机
“砰”!国产新药获批,击穿肺癌靶向
作者:Tony
与欧美人种不同的是,亚洲肺癌患者EGFR突变率高,约达到50%[1],有更多机
 父亲生病一周年小记
2024年3月9日父亲感觉吸气的时候胸部有压迫感去卫生院做了个CT,CT还要经上级医院审
父亲生病一周年小记
2024年3月9日父亲感觉吸气的时候胸部有压迫感去卫生院做了个CT,CT还要经上级医院审
 母亲奥西耐药后应如何选择
2022年10月确诊肺腺癌,基因检测结果EGFR21,服用奥希替尼。2024年6月CT影像检查缓慢
母亲奥西耐药后应如何选择
2022年10月确诊肺腺癌,基因检测结果EGFR21,服用奥希替尼。2024年6月CT影像检查缓慢
 又一个肺癌四代靶向药倒下,奥希替尼
作者:闵
自第一款EGFR-TKI易瑞沙(即吉非替尼)于2005年在我国上市以来,EGFR-TKI药
又一个肺癌四代靶向药倒下,奥希替尼
作者:闵
自第一款EGFR-TKI易瑞沙(即吉非替尼)于2005年在我国上市以来,EGFR-TKI药



 显身卡
显身卡